Dental implants and implantation

Dental implants enable dentist to restore lost teeth without compromising the integrity of healthy adjacent teeth. Dental implants can be used for single or multiple teeth restorations. Dental implants enable dentist to restore edentulous jaws. Dental implants are one of the most advanced treatments’ available to date – about 97% of implants are successfully naturalized and lasts for years. The first dental implant in the world was implanted in the mandibular jaw by Prof. Branemark (Sweden) in 1965. Dental implants are not a novelty, but a time-tested method of tooth restoration, which is experiencing a rapid growth of popularity in Lithuania.
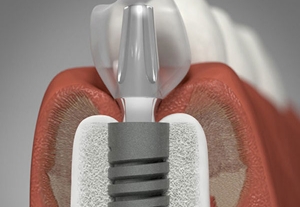
The tooth consists of a crown (tooth part above the gum line) and root (not visible part of the tooth under the gum). Root is in the jaw bone, it keeps the tooth in place. There are many ways to restore the anatomical tooth crown, but only dental implants can fully restore the tooth – both the root and the crown. Dental implants seem to serve and be as comfortable as natural teeth.
A dental implant is a titanium or porcelain screw, which replaces the lost tooth root. Dental implants are placed into the maxillary or mandibular jaw bone and serve as an anchor for dental restoration. When dental implants are fully naturalized, dental crown, bridge or non-removable prosthesis can be made.

A beautiful smile nowadays became a symbol of good health, success and education. Unfortunately, in most cases a beautiful smile is understood only as good looking front teeth. Often missing molar causes no concern, because it is not visible. However, molar teeth play a key role in chewing, maintaining occlusal height, good temporomandibular joint condition and correct adjacent teeth position.
Few missing molars change the profile of the face. Missing teeth affect not only the esthetics, but the general state of health and quality of life. In order to avoid such situations, dental implants are the best solution.
When a tooth is removed, jaw bone resorption starts and adjacent teeth begin to move into the side of the defect. An example could be a bookcase, fully filled with books. If you remove the book, other books collapse in the resulting empty space.
Dental implant will prevent bone resorption and adjacent teeth movement.
Front teeth area to choose aesthetic dental implantation. Coronary part of esthetic dental implants is made of porcelain therefore perfect esthetics can be achieved.
Stages of dental implantation:
- During the first visit, dental implants are placed into the bone and left to engraft for 3-6 months.
- During the second visit, healing caps are placed on the implant, on which dental crown will be made later. Sometimes these healing caps are placed during the first visit, just after the implantation.
- During the third stage, dental crown is manufactured and placed on the implant. The crown is customized in size, shape and color to perfectly match the adjacent teeth. After the restoration is finished, new tooth will not differ from natural teeth.

Sometimes it is possible to perform the dental implantation and dental crown placement in one visit or several days. You can eat and smile immediately after treatment. This is possible, when bone in implant area is thick, implant has good primary stability, the occlusion is correct, occlusal loads are not big.
CEREC CAD/CAM system is the fastest and most reliable way to produce dental prosthesis on implants. Final result is achieved only in one visit. The implant platform position and the supra-implant mucosa outline are transferred into the three-dimensional data set with a digital impression system. Using high-end computer software ceramic restoration is designed, then milled and fixed on the implant.
Pre-operative assessment:
Patient’s general condition is evaluated before dental implantation. Patient is checked for diseases, affecting bone condition (diabetes, rheumatism, multiple sclerosis, tumors, etc.), immune system disorders, cardiovascular diseases (angina pectoris, arrhythmia, hypertension), psychical illnesses, allergic reactions and so on.
Contraindications of dental implants:
Dental implantation is not recommended if recurring oral mucosa diseases and poor oral hygiene are observed, if head and neck radiation therapy was prescribed, also in case of poor anatomical conditions and severe oral pathology. Each case is assessed individually by a dentist.
Types of dental implants:
There are plenty of dental implant systems today. Patients often stumble upon huge price differences and ask which implants to choose. There are about 200 dental implant manufacturers in total. As in any field, there are leaders who have good reputation and are likely to produce a good product. Of course, the famous name is also associated with a higher price.
We use Swiss Straumann dental implants. Straumann are oral implantology pioneers, who implanted the first root-form dental implant 40 years ago. These implants are recognized as one of the best engrafting implants in the world – their success rate is 98-100%. It is scientifically proven, that Straumann implants last the longest. Straumann implant manufacturers give the international warranty for life all over the world.
There are many manufacturers of cheap counterfeits who produce famous brands’ copies of questionable quality. This is not necessarily bad for dental implants, but a manufacturer saves money on researches which in leading companies represent the largest share of the cost. Such savings may not look so bad, but the long-term perspective of such dental implants unfortunately cannot be known. Visually, the implant may not differ from the original, but the implant strength and engraftment highly depends on metal selection (always a special class IV Titan), micropreparation of the surface (which cannot be evaluated without a microscope), sterility of the implant. Therefore in developed countries (e.g. USA) the appropriate service (FDA) does not give the permission to use counterfeits: the authorization is only granted if long-term research has shown that dental implants are safe for the patients and carry out their function properly.
Our advantages:
- All implantations are performed by a qualified and experienced oral surgeon Mindaugas Neverauskas, who specializes in dental implantation for over 10 years, and has performed thousands of implantations.
- We use reliable and internationally recognized implants (Biohorizons, Straumann, Friadent).
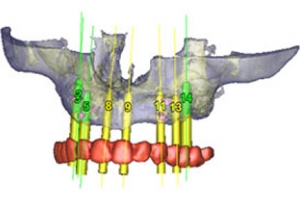
- We perform in-office panoramic X-rays, which is always needed when planning dental implantation.
- If dental implants fail to engraft (which statistically occurs for about 2-3% of patients), our clinic changes them free of charge.
- We use reliable and internationally recognized implants (Biohorizons, Straumann, Dentsply (Xive, Friadent)) at our dental clinic “Pilėnė“ in Vilnius.
One of the most important factors in the outcome of dental implantation is clinician’s competence and experience.
It is necessary to point out that dental crown itself (placed on dental implant) is just as important. Good prosthetics is crucial for good final outcome.
To find out the cost of dental implants click here.